


Celebrating Sickle Cell Cure, with Caution
A major advance in gene therapies now calls for healthcare delivery systems to catch up and develop ways to equitably and justly deliver high quality care to ALL people affected by sickle cell


A Miracle of Modern Science after Nearly 75 years
Recently, the FDA announced the approval of two gene therapies for sickle cell disease!
This long awaited miracle of modern science deserves to be celebrated. The road from November 25, 1949, when the molecular origins of sickle cell disease (SCD) were discovered (1), to Dec 8, 2023, when the FDA approved the first two gene therapies for sickle cell is a glorious victory of collective human ingenuity. (2)
It is an important moment to honor the hundreds of scientists, including two inspiring women in science (Emmanuelle Charpentier and Jennifer Daoudna, who won the 2020 Nobel prize for CRISPR gene-editting technology underpinning one of the two therapies), researchers, clinicians, and most importantly clinical trial volunteers and patient advocates who have worked hard, sacrificed, and in the case of the clinical trial volunteers, literally risked their lives, over decades to get our society to this moment. Collaborative, open science in thoughtful and engaged dialogue with patient advocates has won the day.
And yet, the celebration is tainted with a note of caution, particularly around equitable access to care. This reality has stained sickle cell care delivery for decades, but it becomes all the more acute with the promise of these novel therapies.

America’s Tainted Sickle Cell Care History
No clear-eyed analysis about care for people affected by sickle cell in the United States, can start without first acknowledging systemic racism. As Medical Director of the Adult Sickle Cell Center at Yale and professor of medicine, Dr. Cecelia Calhoun, so clearly stated on the Health and Veritas podcast, “because of the transatlantic slave trade, we are here.” (4)
Sickle cell disease is part of a set of closely related genetic diseases (hemoglobinopathies) that are evolutionarily more common in populations that have, over distant human history, resided in Malaria endemic areas. Peoples with roots in Africa, Southeast Asia, and some areas of the Mediterranean (Greece, Cyprus, Italy) will have a greater probably of carrying the sickle cell genes (2). In the United States, this means 91% of people with sickle cell disease identify their race as black, 4% as Hispanic, and only 3% as white (3). Thus for America, the dark history of ongoing systemic racism against black people and racialized medicine is intricately linked to the neglectful and fragmented care people with sickle cell receive as a whole.
The main symptom of sickle cell disease is pain. To imagine the pain of sickle cell it helps to understand that what is literally happening during a sickle cell vaso-occlusive crisis is physiologically the same as a thousand heart attacks, deep in the marrow of a person’s bones, happening at once. If this weren’t bad enough, too many patients with sickle cell disease have to endure the additional pain of not being believed when they tell their care providers about their symptoms, labelled inappropriately as “opiate seeking”, and too often having evidence-based treatment either delayed or denied (5). There also just aren’t enough clinics and emergency departments well versed and experienced with treating sickle cell patients in either acute or preventative settings. These missed opportunities for timely and evidence-based care contribute to irreversible and debilitating sequelae, such as: splenic sequestration, life-threatening acute chest crises, necrosis of the hip, kidney failure, and strokes, in otherwise generally young and healthy people.

Image: Art of the late Hertz Nazaire, Connecticut artist and sickle cell warrior (6).
So while sickle cell disease is devastating due to the unlucky genetic dice roll of evolution, with modern comprehensive care, even in the pre-gene therapy era, it should not be as devastating as it currently is. We have our dysfunctional human made systems to thank for that. There are evidence-based guidelines for sickle cell care (likely to updated soon in light of new therapeutics), that if followed consistently, would mitigate a massive amount of the pain and suffering (and total cost of care) that people and families affected by sickle cell currently endure (7). The access and social justice problem associated with sickle cell care is as much a part of the issue as the genetic problem.
While the new gene therapies address the core genetic problem, they do not address the core social problem. We must ensure this historical scientific moment is leveraged to address both.
Gene Therapy Sticker Shock
Sickle cell gene therapy is not cheap.
Bluebird Bio priced Lyfgenia at $3.1 million. Vertex Pharmaceutical’s version of the gene therapy, Casgevy, is priced a $2.2 million (8). For perspective, the average total wealth of an African American family in the United States is a mere $44,900 (9).
Younger versions of ourselves would have railed against the “pharma companies’ greed” and demanded they lower their prices. But as we’ve grown older (and hopefully wiser) we’ve come to find such rhetoric, while emotionally cathartic, is rarely effective in actually getting people the care they need.
The truth is gene therapy, until this moment, was an untested, and very unlikely to work, novel technology in medicine. Without investors, including institutional investors like pension funds, taking massive financial risks to fund the two startups that have got us here, Bluebird Bio and CRISPR Therapeutics (in partnership with Vertex Pharmaceuticals), we wouldn’t even be able to have this conversation.
It is likely that something on the order of $100 Billion of private capital has been invested in developing gene therapy for rare diseases like SCD in the last decade (10). This is amazing. It is unrealistic to ask these private investors to not seek a return on that very patient and risky investment by pricing these therapies at what “the market can bear.”
But the market can only bear these high prices because sickle cell, in its current state of uncoordinated treatment and fragmented care, currently costs Medicaid and Medicare on average $42,000 per patient per year (r). To put that in context that’s over twice the average per patient per year cost of congestive heart failure, one of America’s most costly chronic conditions. The bulk of people with sickle cell, if they have any insurance at all (!), are covered by Medicaid or Medicare or both. Over the lifetime of a person with sickle cell disease, the total cost of care for their condition to government health insurance programs is many fold higher than the $3 million one time gene therapy cost. From the perspective of the insurer and the tax-paying public, the $3 million is actually a really good investment.
Except sickle cell is so common in some states that a 2019 JAMA Pediatrics analysis showed that gene therapy given to just 7% of the total sickle cell population (the assumed eligible population based on current bone marrow transplant eligibility guidelines) could bankrupt the entire Medicaid programs of 10 US states! ( And that analysis estimated the price of gene therapies at nearly half the recently announced prices from Vertex and Bluebird Bio!
Also, these therapies are also not without real physical risks and consequences for patients. Gene therapy is essentially a bone marrow transplant using your own genetically edited cells, and includes all the risks and side effects of that complex procedure including immune suppression and potential infertility. Bluebird Bio’s non-CRISPR based method also carries a black box warning that patients need to be screened for life for rare and difficult to treat cancers after the treatment, which prior to CRISPR was the main reason gene therapy struggled to get off the lab bench into the clinic.
Gene therapy is a very dramatic therapy that really should be reserved for only the absolute most severe cases of sickle cell disease.
In truth, the gene therapies really only apply to about 7% of people affected by sickle cell (at this point). For the other 93%, there are increasingly effective non-gene therapy treatments available, including good old fashion hydroxyurea and use of outpatient day hospitals and infusion centers instead of ED in acute setting. The major barrier to people accessing these therapies is our fragmented health system. Advanced primary care, care coordination, telehealth, and complex care models are the key to just sickle cell care. They become even more important in post-gene therapy era.
The way to mitigate the cost barrier for gene therapy for the small percentage of people with the most severe forms of sickle cell, is to lower the population level cost of care while improving outcomes for all patients affected by sickle cell.
Reaching the Hardest to Reach
There is also a massive geographic component to fragmented care, in addition to the financial access question.
Most people affected by sickle cell live in either in New York City, Chicago, the mid-Atlantic urban centers, or the rural Southeast. Yet, the location of the gene therapy treatment centers don’t match this distribution.
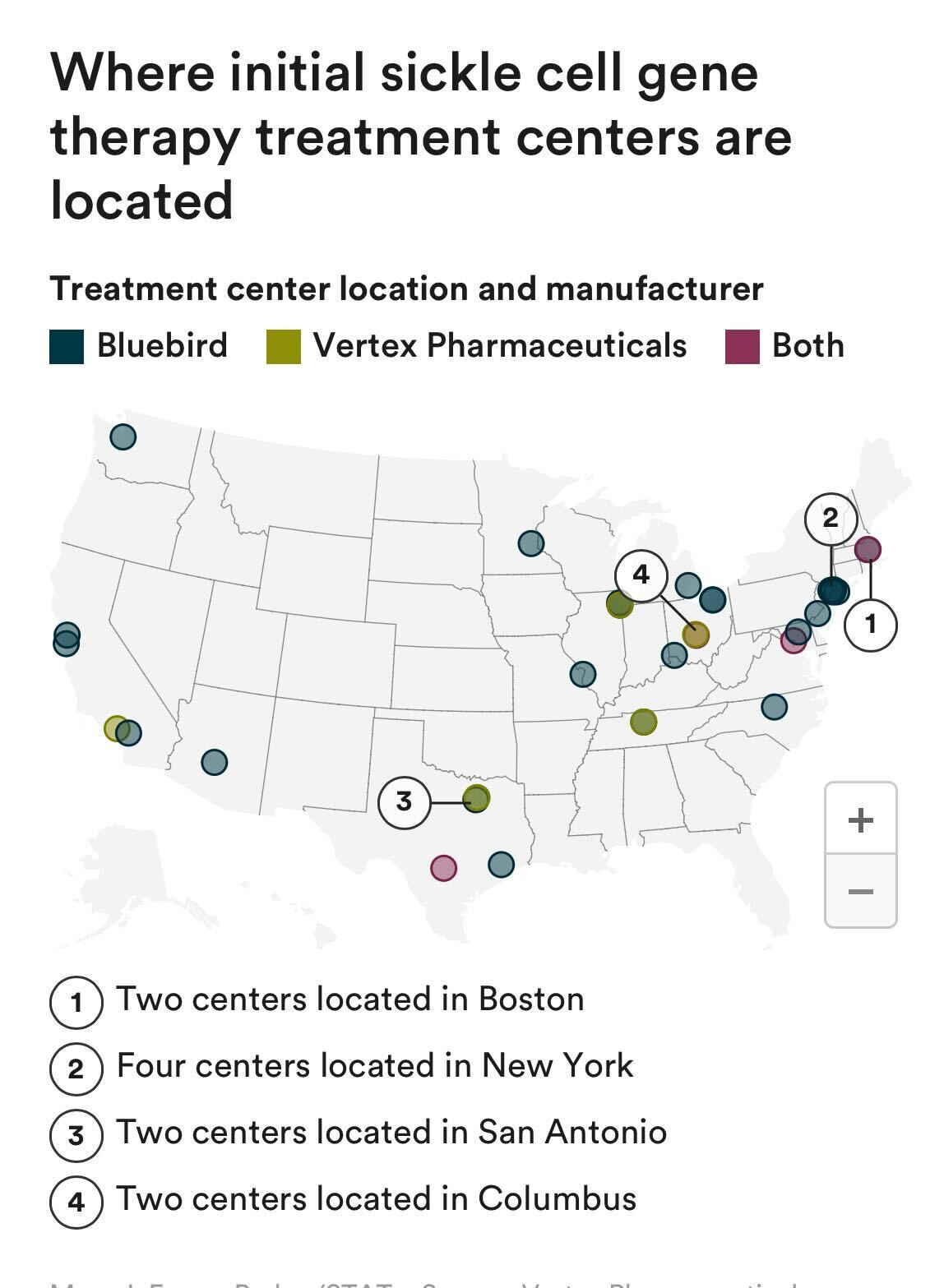
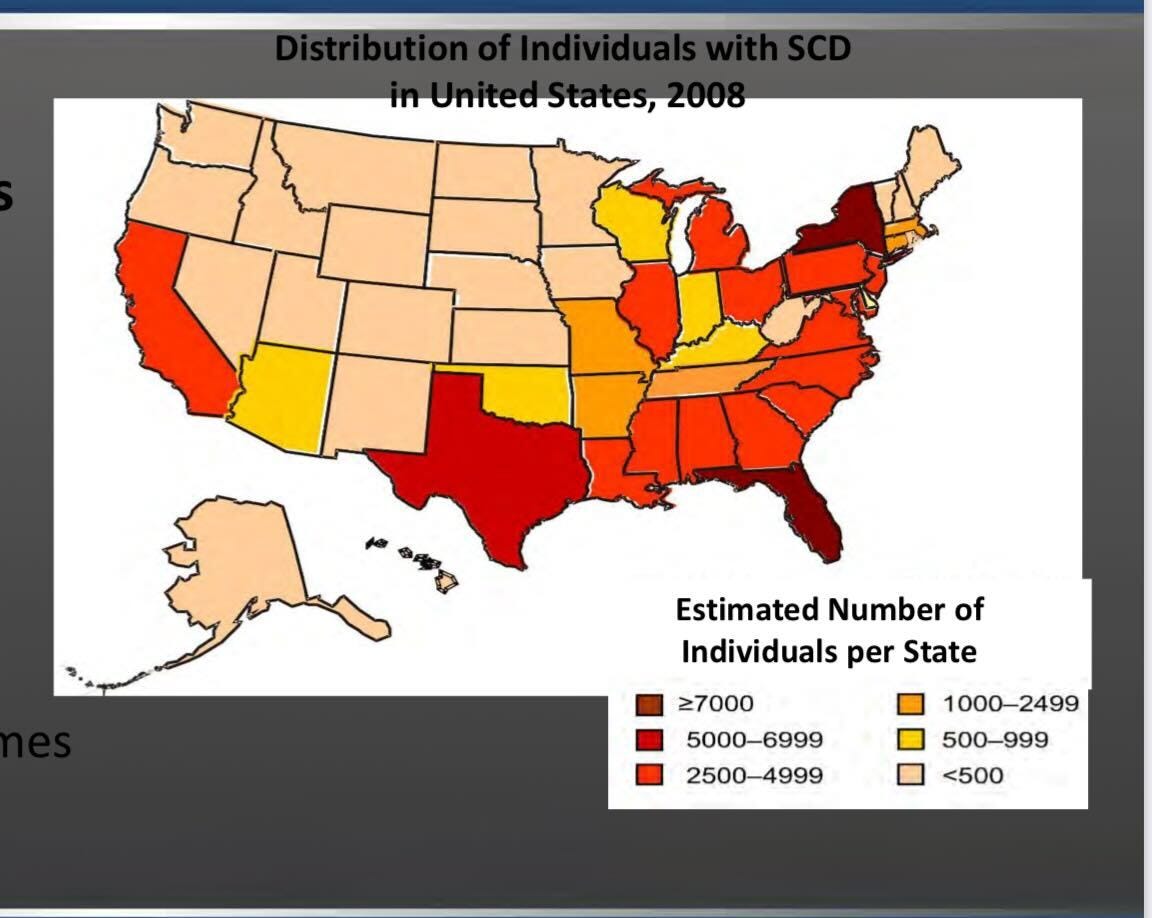
In a 2012 CMS analysis (4), Massachusetts has a mere 877 Medicaid beneficiaries affected by Sickle Cell Disease (SCD), while Florida had 5,395, Georgia had 3,752, and Alabama had 1,754.
Yet, Boston now hosts two sickle cell gene therapy centers, while those 3 contiguous states, with significantly larger populations affected by SCD— Florida, Georgia and Alabama — have none. It is fantastic that the 877 Medicaid beneficiaries with SCD in the Boston area have reasonable access to and choice between two separate treatment facilities in their community, but what of the tens of thousands of people affected by sickle cell that happen to live closer to Miami, Atlanta, or Birmingham?
Granted both Vertex and Bluebird state they are currently preparing to open new centers, and we anticipate many of those will be in the Southeast. Yet, the striking disconnect between where the most advanced therapies for sickle cell are currently available and where the need is greatest, illustrates a larger point that has plagued the sickle cell community for decades. The best care is not necessarily available to the population centers that need it most.
The access and social justice problem associated with sickle cell care is as much a part of the issue as the genetic problem.
Even in this most Mendelian of genetic diseases, a person's clinical outcomes are more deeply affected by their zip code than their genetic code.
People in rural communities, those who live far from large academic medical centers, or those who live in states without robust sickle cell programs, are even more isolated and forgotten than the baseline neglect that our nation’s care delivery system has collectively shown people affected by sickle cell.
Applying What We Know Already Works to SCD
Now that the greatest scientific advance in history for people affected by genetic disease is available on the market, it is time to build equally historic social and care delivery advancements for those with chronic complex conditions.
Advances at the bench, without equal advances at the bedside and the sidewalk are no advancement at all.
(For those less familiar with medical academic speak: bench=scientific research, bedside= care delivery, and sidewalk= social determinants of health… this last one we just coined).
One of us (Dr. O’Brien) has spend the last decade developing and leading high-touch, team-oriented, advanced primary care models for populations of people with a variety of complex chronic conditions, focused on advancing care at the bedside and the sidewalk.
What we have learned, and the data support, is that well designed programs that combine technology to enable multi-disciplinary teams, population-based analytics, guideline directed evidence-based care, and novel locations of delivery including virtual care, hybrid virtual care, and home visits, can dramatically improve patient outcomes across various complex conditions and population groups.
There is good reason to believe these strategies applied to complex disease populations, like those affected by sickle cell, would ensure that those who qualify from novel gene therapies can actually access this treatment, and those who don’t, still receive the best possible care and quality of life that decades of non-gene-therapy advancements and good old fashion social care provide. These care models, especially those with a heavy emphasis on telehealth, are particularly effective for the exact subpopulations in greatest need for improved access, rural and low-income communities, without direct access to an academic medical center.

The time is now.
All people affected by sickle cell (and all rare and complex conditions for that matter) deserve a life free of pain, debility, and avoidable hospitalizations, even if they don’t qualify for or elect not to pursue novel gene therapies or bone marrow transplant.
People, families, and communities affected by sickle cell have been ignored for too long. We can’t miss this rare moment of public acknowledgement of their needs to improve the lives of all people affected by America’s most common serious genetic disorder.
References:
https://www.science.org/doi/10.1126/science.110.2865.543
https://www.statnews.com/2023/12/08/fda-approves-casgevy-crispr-based-medicine-for-treatment-of-sickle-cell-disease/
https://www.nature.com/scitable/topicpage/natural-selection-uncovering-mechanisms-of-evolutionary-adaptation-34539/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7669607/
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2734070
https://www.ctpublic.org/arts-culture/2021-11-02/artist-sickle-cell-warrior-hertz-nazaire-dies-at-48
https://www.hematology.org/education/clinicians/guidelines-and-quality-care/clinical-practice-guidelines/sickle-cell-disease-guidelines.
https://www.biopharmadive.com/news/crispr-sickle-cell-price-millions-gene-therapy-vertex-bluebird/702066
https://www.federalreserve.gov/econres/notes/feds-notes/greater-wealth-greater-uncertainty-changes-in-racial-inequality-in-the-survey-of-consumer-finances-20231018.html#fig1
https://www.biopharmadive.com/news/gene-cell-therapy-funding-2020-arm-report/596790/
 | A guest post by
|